
Statin Tolerance & Risk Calculator
Your Profile
Select your genetic profile and current or intended medication.
Analysis Result
Select your details and click "Analyze Compatibility" to see results.
Alternative Statin Guide
| Statin | Transporter Dependence | Suitability for High Risk (CC) |
|---|
Imagine taking a medication that could save your life from a heart attack, only to have it wreck your muscles with pain and weakness. For millions of people, this is the reality of statin intolerance. You are told you need a statin to lower your cholesterol and protect your heart, but within weeks or months, you develop muscle aches, fatigue, or even severe damage. The standard advice? Stop the drug, try a lower dose, or switch brands. But what if the problem isn't the brand, or the dose, but your own DNA?
This is where pharmacogenomics enters the picture. It is not just buzzword-heavy science; it is a practical tool that looks at how your genes process medications. Specifically, for statins, it can tell you why your body reacts poorly to certain drugs and which ones might work without the painful side effects. If you have struggled with statins in the past, understanding your genetic profile might be the missing piece that allows you to stay on treatment safely.
Why Do Some People Get Muscle Pain From Statins?
Statins are incredibly effective. They block an enzyme called HMG-CoA reductase, which helps your liver make cholesterol. This lowers LDL (bad) cholesterol and reduces the risk of heart disease and stroke. However, about 7% to 29% of patients report muscle-related issues, ranging from mild aches to severe myopathy. Doctors call this Statin-Associated Muscle Symptoms (SAMS).
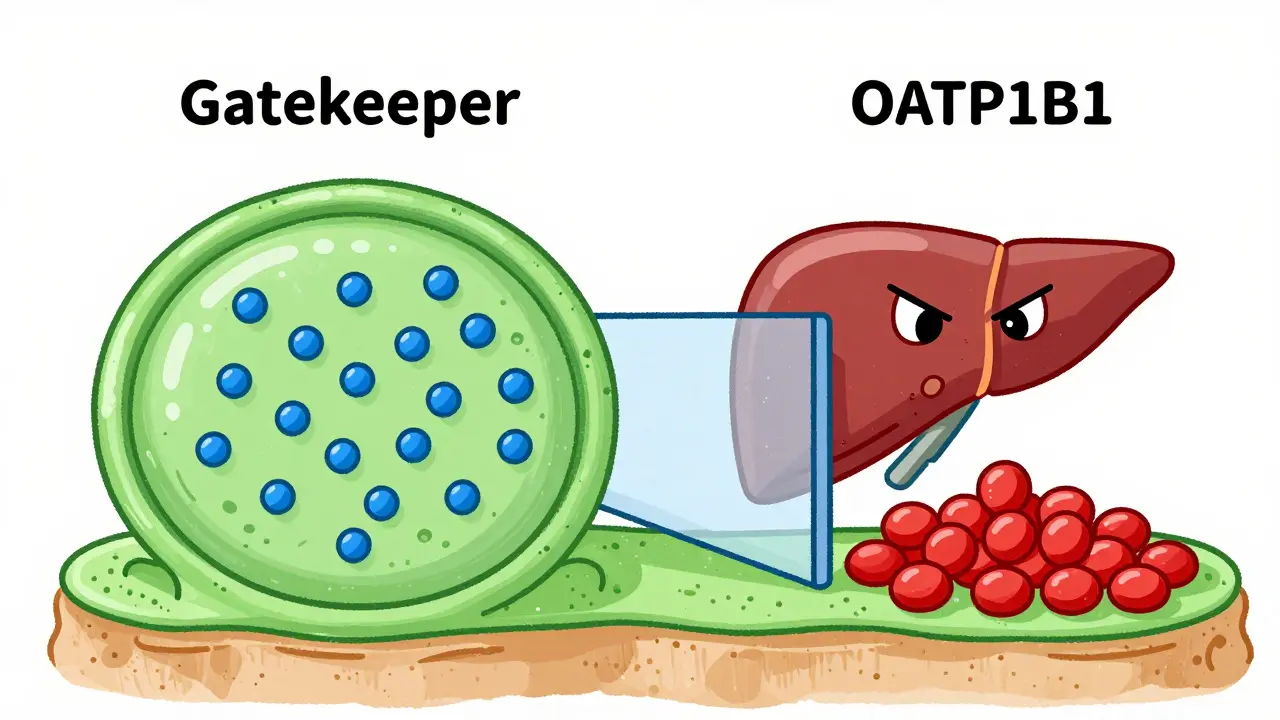
For a long time, doctors didn't know exactly why some people got SAMS while others took high doses without a twinge. We knew it wasn't random. It turns out, genetics play a huge role. Your liver uses specific transporters to move statins into cells so they can do their job. If those transporters are slow or broken due to a genetic variant, the statin builds up in your bloodstream instead of staying in the liver. Higher levels of the drug in your blood mean more exposure to your muscles, leading to toxicity and pain.
The key player here is SLCO1B1, a gene that provides instructions for making a protein called OATP1B1. This protein acts like a gatekeeper on the surface of liver cells, pulling statins out of the blood and into the liver. When this gate works well, statin levels in the rest of your body stay low. When it doesn't, the drug circulates freely, increasing the risk of muscle damage significantly.
The SLCO1B1 Gene: The Main Suspect
If you look at research on statin tolerance, one name comes up again and again: the SLCO1B1 gene. A landmark study published in the New England Journal of Medicine in 2008 identified a specific variation in this gene, known as rs4149056, as a major cause of simvastatin-induced myopathy.
Here is how the genetics break down:
- TT Genotype (Common): About 83% of people with European ancestry have two normal copies of this gene. Their liver gates work efficiently. They tolerate simvastatin well.
- TC Genotype (Heterozygous): About 15% of people have one normal copy and one variant copy. Their liver uptake is reduced, leading to higher drug levels in the blood. They have a moderately increased risk of muscle symptoms.
- CC Genotype (Rare but High Risk): About 1-2% of people have two variant copies. Their liver uptake is very poor. Studies show these individuals have a 4.5-fold increased risk of severe myopathy when taking high-dose simvastatin (80mg).
This isn't just theory. The Clinical Pharmacogenetics Implementation Consortium (CPIC), a group of experts who translate genetic data into clinical guidelines, has issued strong recommendations based on this. They advise that clinicians should avoid prescribing simvastatin 80mg to anyone with the CC genotype. For TC carriers, they suggest using lower doses or switching to a different statin entirely.
Does This Apply to All Statins?
This is a critical distinction that many patients miss. The SLCO1B1 gene primarily affects statins that rely heavily on the OATP1B1 transporter to enter the liver. Simvastatin is the most dependent on this pathway. Atorvastatin also uses it, but to a lesser extent. Rosuvastatin, pravastatin, and fluvastatin use different pathways or are less affected by this specific genetic variant.
In fact, recent large-scale studies, including one published in Circulation: Genomic and Precision Medicine in 2021, found no significant association between the SLCO1B1 variant and muscle symptoms for atorvastatin or rosuvastatin. This means if you are a CC carrier, you aren't doomed to never take a statin. You just need to avoid the ones that get stuck in your blood. Pravastatin, for example, bypasses the OATP1B1 transporter almost entirely. For someone with the high-risk CC genotype, switching from simvastatin to pravastatin can reduce myopathy risk by up to 80% while still lowering cholesterol effectively.
| Statin Name | Dependence on SLCO1B1 Transporter | Risk for CC Genotype Carriers | Recommendation for High-Risk Patients |
|---|---|---|---|
| Simvastatin | High | Very High (4.5x risk) | Avoid, especially at high doses |
| Atorvastatin | Moderate | Moderate | Use with caution or lower doses |
| Rosuvastatin | Low | Low | Generally safe alternative |
| Pravastatin | Minimal | Very Low | Preferred alternative for intolerant patients |
| Fluvastatin | Minimal | Very Low | Preferred alternative for intolerant patients |
Other Genetic Factors Beyond SLCO1B1
While SLCO1B1 is the star of the show, it is not the only actor. Research continues to uncover other genes involved in statin metabolism and muscle sensitivity. For instance, the CYP2D6 and CYP3A4 enzymes help break down certain statins. If you have variants that make you a "poor metabolizer," your body clears the drug slower, leading to higher concentrations over time. About 7-10% of Caucasians carry poor metabolizer variants for CYP2D6.
Other genes like ABCB1 (which pumps drugs out of cells) and ABCG2 have been studied, though their impact is less clear-cut than SLCO1B1. More recently, researchers identified associations with GATM and CACNA1S, which relate to muscle function itself rather than drug transport. This suggests that for some people, the issue isn't just too much drug in the system, but a genetic predisposition to muscle injury when exposed to any stressor, including statins. Understanding this complexity is why comprehensive pharmacogenomic panels are becoming more popular than single-gene tests.
Should You Get Tested? The Pros and Cons
The decision to undergo pharmacogenomics testing is personal, but the data offers some clarity. On the positive side, real-world experiences show promise. A survey of patients at Mayo Clinic found that 78% of those with prior statin intolerance were successfully restarted on a statin after receiving genotype-guided recommendations. That is a massive improvement over historical controls, where only 58% succeeded. Imagine going from a coin flip to a near-certainty of finding a medication that works.
However, there are hurdles. Cost and insurance coverage remain significant barriers. As of 2023, out-of-pocket costs for standalone SLCO1B1 testing ranged from $150 to $400, and only about 28% of commercial insurers covered it routinely. Medicare coverage is limited to specific circumstances. Additionally, not all doctors are comfortable interpreting these results. A 2021 survey revealed that 34% of primary care physicians felt unprepared to interpret pharmacogenomic reports without specialized software support. This gap between available technology and clinical readiness can leave patients confused after receiving their results.
There is also the question of utility. A 2020 randomized trial in JAMA Network Open found that simply providing SLCO1B1 results to physicians did not significantly improve adherence or reduce muscle symptoms compared to usual care. Critics argue that we don't yet have enough evidence to prove that testing saves lives or prevents heart attacks better than the current "trial and error" method. Supporters counter that trial and error often leads to patients quitting statins altogether, leaving them unprotected against cardiovascular disease.
How to Navigate Testing and Treatment
If you are considering testing, here is a practical roadmap. First, talk to your doctor about your history of muscle pain. If you have tried multiple statins and failed, ask if pharmacogenomics testing is appropriate for you. Look for labs that are CLIA-certified, such as Mayo Clinic Laboratories or ARUP Laboratories, to ensure accuracy.
When you get your results, focus on actionable information. If you are an SLCO1B1 CC carrier, discuss switching to pravastatin or rosuvastatin immediately. If you are a TC carrier, consider starting with a low dose of a non-SLCO1B1-dependent statin. Use resources like the NIH Pharmacogenomics Knowledgebase (PharmGKB) to verify the evidence levels behind the recommendations. Remember, the goal is not just to find a statin you can tolerate, but to find one that effectively lowers your LDL to target levels. Genetic testing is a tool, not a cure-all. It guides the choice, but regular monitoring of your cholesterol and liver enzymes remains essential.
The future of this field looks bright. Polygenic risk scores, which combine dozens of genetic variants, are being developed to predict statin response with greater accuracy than single-gene tests. Early studies suggest these combined scores could significantly improve prediction models. As healthcare systems integrate genomic data into electronic health records, the hope is that your genetic profile will automatically flag high-risk combinations before you ever take a pill, preventing side effects before they start.
What is the best statin for someone with the SLCO1B1 CC genotype?
For individuals with the SLCO1B1 CC genotype, pravastatin and fluvastatin are generally considered the safest options because they do not rely heavily on the OATP1B1 transporter for uptake into the liver. Rosuvastatin is also a viable alternative as it has minimal interaction with this specific genetic variant. Simvastatin should typically be avoided, especially at high doses.
Does insurance cover pharmacogenomics testing for statins?
Coverage varies widely. As of recent data, only about 28% of commercial insurers routinely cover SLCO1B1 testing. Medicare coverage is limited to specific molecular diagnostic programs. Many patients may need to pay out-of-pocket, with costs ranging from $150 to $400 for standalone tests. It is crucial to check with your specific provider and request pre-authorization if possible.
Can I take any statin if I have the TC genotype?
Yes, but with caution. The TC genotype carries a moderate risk of muscle symptoms, particularly with simvastatin. Clinicians often recommend starting with lower doses of simvastatin or choosing alternative statins like atorvastatin or rosuvastatin. Monitoring for muscle pain is essential when initiating therapy.
How long does it take to get results from a pharmacogenomics test?
Turnaround times typically range from 5 to 10 business days after the sample (usually a buccal swab or blood draw) reaches the laboratory. Some direct-to-consumer kits may take slightly longer due to shipping and processing logistics.
Is pharmacogenomics testing recommended for everyone starting statins?
Currently, major guidelines like those from the American College of Cardiology do not recommend routine testing for all patients starting statins. It is most strongly considered for patients who have previously experienced statin intolerance or muscle symptoms, helping to guide re-challenge strategies or alternative selections.



Terrence spry
I'm a pharmaceutical scientist specializing in clinical pharmacology and drug safety. I publish concise, evidence-based articles that unpack disease mechanisms and compare medications with viable alternatives to help readers have informed conversations with their clinicians. In my day job, I lead cross-functional teams advancing small-molecule therapies from IND through late-stage trials.
view all posts