When dealing with Amiodarone, a class III anti‑arrhythmic medication used to control serious heart rhythm problems. Also known as Cordarone, it is a type of anti‑arrhythmic drug, medications that stabilize the electrical activity of the heart and is commonly prescribed for atrial fibrillation, an irregular, often rapid heart rate that can cause poor blood flow. Amiodarone is powerful enough to reset dangerous rhythms, yet it demands careful handling because it sticks around in the body for weeks.
One of the main reasons doctors reach for amiodarone is its ability to terminate ventricular tachycardia and prevent ventricular fibrillation, two life‑threatening patterns that can lead to sudden cardiac death. The drug works by prolonging the cardiac action potential, which slows the heart’s electrical conduction and gives the heart a chance to restart in a normal rhythm. Because it influences many ion channels, amiodarone also dampens abnormal impulses that arise from the atria or ventricles, making it a go‑to option when other anti‑arrhythmics fall short.
Before starting therapy, clinicians review a patient’s existing conditions because amiodarone interacts with a long list of other medicines. Common culprits include warfarin, statins, and certain antidepressants; these combos can raise the risk of bleeding, muscle problems, or altered drug levels. Another crucial factor is the drug’s impact on the thyroid. Amiodarone contains iodine, which can trigger both hypothyroidism and hyperthyroidism, so regular blood tests are a must. The lungs are also on the radar—pulmonary toxicity may develop slowly, presenting as shortness of breath or a persistent cough, especially after high‑dose or long‑term use.
Dosing usually begins with a loading phase—often 800‑1200 mg per day for a week—to quickly achieve therapeutic levels, followed by a maintenance dose of 100‑200 mg daily. The exact amount depends on the rhythm being treated, the patient’s weight, and kidney or liver function. Because the drug’s half‑life stretches up to several weeks, any dosage change takes time to show effect, which is why doctors monitor ECGs, liver enzymes, and kidney markers regularly during the first few months.
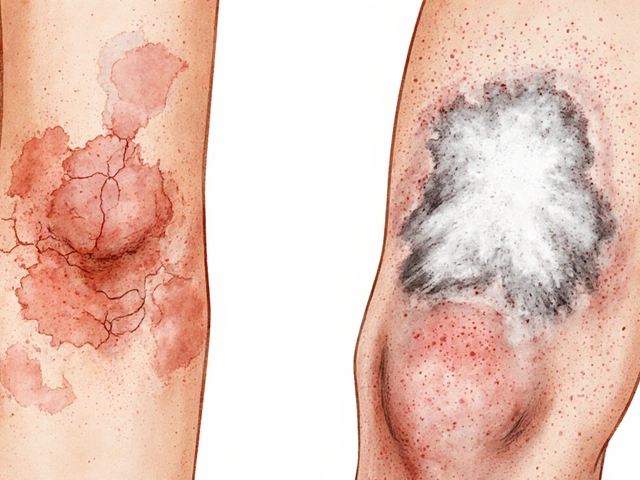
Patients often ask how to recognize side‑effects early. Look for skin discoloration (a blue‑gray hue), photosensitivity, or blotchy rashes—signals that the skin is storing the drug. Vision changes, such as blurred sight or a halo around lights, may hint at corneal deposits. If you notice new shortness of breath, unexplained weight gain, or persistent fatigue, contact your healthcare provider right away; these could be early signs of lung involvement.
While amiodarone is effective, it isn’t the first‑line choice for every arrhythmia. For less severe atrial fibrillation, doctors may start with beta‑blockers, calcium channel blockers, or newer anti‑arrhythmics that have a shorter half‑life and fewer organ‑specific risks. However, when the rhythm issue is refractory or the patient has structural heart disease, amiodarone often becomes the most reliable option because it works across multiple rhythm pathways.
Understanding the balance between benefit and risk is essential. A thorough baseline work‑up—including thyroid panels, liver function tests, chest X‑ray, and pulmonary function tests—sets the stage for safe therapy. Ongoing monitoring every 3‑6 months helps catch problems before they become serious, allowing dosage tweaks or a switch to another medication if needed.
Below you’ll find a curated collection of articles that dive deeper into topics like drug‑drug interactions, specific dosing strategies for various heart conditions, and patient stories that illustrate real‑world management of amiodarone therapy. Whether you’re a patient looking for practical tips or a practitioner needing a quick refresher, the posts ahead will give you actionable insights to navigate this powerful medication confidently.
Explore how amiodarone works for catecholaminergic polymorphic ventricular tachycardia, its dosing, side effects, and how it compares with beta‑blockers, flecainide, and ICDs.
read more