Antibiotic Liver Injury Pattern Analyzer
Please enter values to calculate.
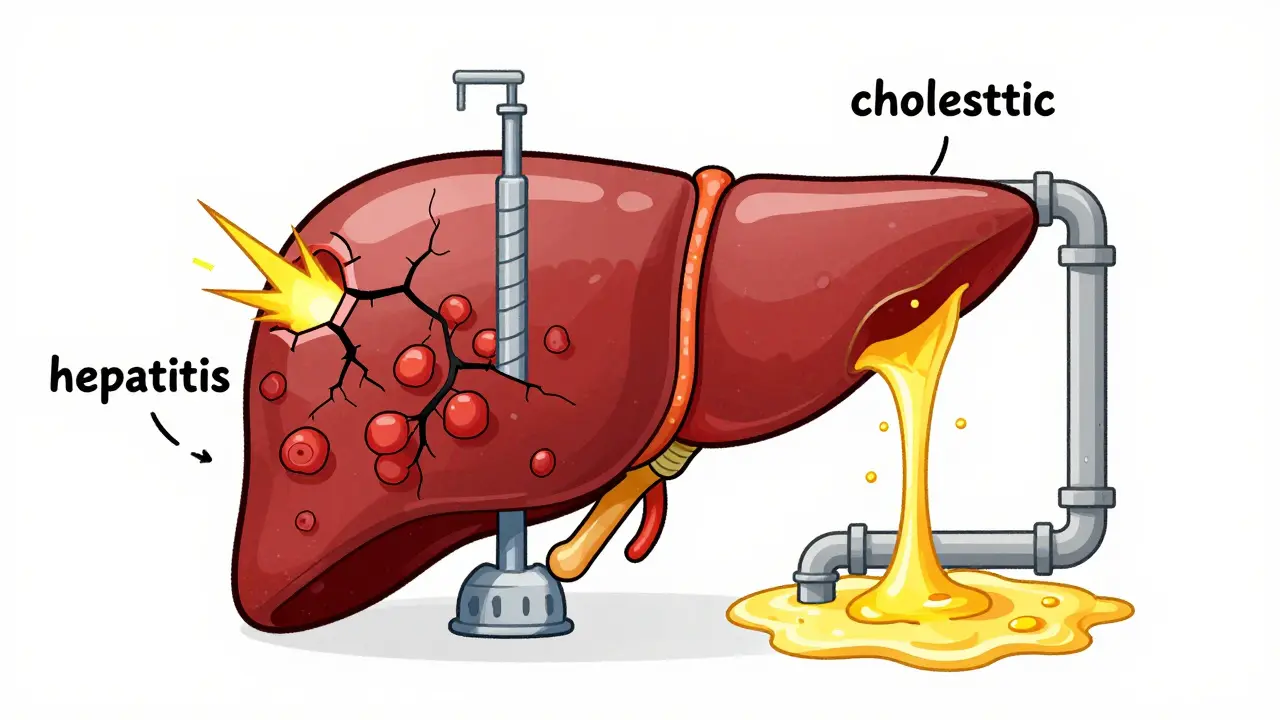
• R > 5: Hepatocellular (Hepatitis-like)
• R < 2: Cholestatic (Bile-flow obstruction)
• 2 ≤ R ≤ 5: Mixed Pattern
Taking a course of antibiotics is a common experience, but for some, the medicine meant to kill bacteria triggers an unexpected attack on the liver. This is known as antibiotic-related liver injury is a specific form of drug-induced liver injury (DILI) where antibiotic medications cause hepatic inflammation or bile flow obstruction. It isn't just a rare side effect; in intensive care settings, antibiotics are linked to about 64% of all drug-induced liver injury cases. Whether it's a simple ear infection treatment or a heavy-duty ICU regimen, the risk varies wildly depending on the drug, the dose, and your own genetics.
| Pattern Type | Primary Marker | Common Example | Typical Onset |
|---|---|---|---|
| Hepatocellular (Hepatitis) | High ALT (>5x ULN) | Mixed (varies by drug) | Days to Weeks |
| Cholestatic | High ALP (>2x ULN) | Amoxicillin-clavulanate | 1-6 Weeks |
| Mixed | Both ALT & ALP High | Ciprofloxacin | 1-2 Weeks |
The Two Faces of Liver Injury: Hepatitis vs. Cholestasis
When a doctor looks at your blood work, they aren't just looking for "liver issues"-they are looking for a specific pattern. The liver usually reacts to antibiotics in one of two ways: hepatocellular injury (which looks like hepatitis) or cholestatic injury.
Hepatocellular injury happens when the actual liver cells, the hepatocytes, are damaged. This shows up as a spike in Alanine Aminotransferase (ALT), an enzyme that leaks into the blood when cells break open. On the flip side, cholestatic injury is more about the "plumbing." It occurs when the flow of bile is blocked or slowed down, causing Alkaline Phosphatase (ALP) to climb. To figure out which one is happening, clinicians use the "R-ratio." If the ratio of ALT to ALP is greater than 5, it's hepatocellular; if it's less than 2, it's cholestatic. Anything in between is a mixed bag.
Why Does This Happen? The Biological Trigger
It isn't just the drug itself hitting the liver; often, it's a chain reaction starting in the gut. Gut microbiota dysbiosis is a key driver here. Antibiotics wipe out both bad and good bacteria. When the good bacteria vanish, the intestinal barrier can weaken, allowing toxins to leak into the bloodstream and head straight to the liver.
Once inside the liver, the damage happens at the cellular level. Many antibiotics cause mitochondrial dysfunction. Think of the mitochondria as the cell's power plant; when antibiotics disrupt them, they produce reactive oxygen species (ROS) that act like chemical sandpaper, wearing down the cell from the inside. In some cases, the body creates a "reactive metabolite"-a toxic byproduct of the drug's metabolism-that binds to liver proteins and triggers an immune response.
High-Risk Antibiotics You Should Know
Not all antibiotics are created equal. Some are practically benign to the liver, while others are notorious for causing issues. Amoxicillin-clavulanate is perhaps the most famous offender, particularly for causing cholestatic injury. It's listed as a high-risk medication by the LiverTox database, with a significant number of cases reported per 100,000 prescriptions.
In the ICU, the stakes are higher. A combination called Tazobactam/piperacillin (TZP) has a concerning track record. In some studies, nearly 29% of patients receiving TZP for a week or more developed liver injury. Interestingly, other strong antibiotics like Meropenem also cause injury, but research shows men are about 2.4 times more likely to experience this than women.
Identifying the Red Flags: Symptoms and Lab Work
The tricky part about antibiotic-related liver injury is that it doesn't always start with a bang. Some patients have "silent" injury, where their liver enzymes spike but they feel perfectly fine. However, when symptoms do appear, they can be severe:
- Yellowing of the skin and eyes (jaundice)
- Deep fatigue and sudden weakness
- Nausea and a total loss of appetite
- Dark-colored urine
For clinicians, the timing is a huge clue. If you're taking a beta-lactam (like amoxicillin), the injury often creeps up 1 to 6 weeks after you start. Fluoroquinolones, however, can hit much faster, sometimes within the first 7 to 14 days. There is also a clear link to the duration of treatment; taking an antibiotic for 7 days or more can increase your risk of liver injury by over 3 times compared to a short 3-day burst.
How Doctors Manage and Prevent Injury
Managing this is a balancing act. You can't always just stop the antibiotic if the patient is fighting a life-threatening infection. Most doctors follow the "rule of 5": if ALT exceeds 5 times the upper limit of normal (ULN) or ALP exceeds 2 times the ULN along with symptoms, it's usually time to switch medications.
Prevention starts with baseline testing. Getting a liver function test (LFT) before starting a high-risk drug allows doctors to see if the liver is already stressed. For patients in the ICU or those on long-term courses, weekly monitoring is the gold standard to catch the slide toward failure before it becomes irreversible.

The Future of Liver Safety: Genetics and Probiotics
We are moving away from a one-size-fits-all approach. New research into Human Leukocyte Antigen (HLA) associations suggests that some people are genetically predisposed to liver injury. In a few years, a simple genetic test might tell your doctor exactly which antibiotic to avoid to keep your liver safe.
There is also a push to protect the gut. Since dysbiosis triggers so much of the damage, clinical trials are currently testing whether taking specific probiotics during antibiotic therapy can prevent the intestinal leak and protect the liver. Early data suggests that maintaining a healthy population of Faecalibacterium prausnitzii in the gut could significantly lower the risk of injury.
Does every antibiotic cause liver damage?
No. Most antibiotics are safe for the liver. Risk is categorized by databases like LiverTox, where only a small percentage are labeled "high-risk." Most people tolerate antibiotics without any hepatic issues.
How can I tell if my antibiotic is affecting my liver?
Look for jaundice (yellowing of eyes/skin), dark urine, and extreme fatigue. However, because these can mimic the infection you're treating, a blood test for ALT and ALP levels is the only definitive way to know.
Will my liver recover after I stop the medication?
In the vast majority of drug-induced liver injury cases, the liver recovers fully once the offending drug is discontinued. However, severe cases of hepatocellular necrosis may require supportive care or hospitalization.
Why do some people get liver injury while others don't?
It's a mix of genetics (HLA markers), the state of your gut microbiome, and other health factors. For example, patients with sepsis have a 1.8-fold higher risk of developing liver injury during antibiotic therapy.
What is the "R-ratio" used for?
The R-ratio helps doctors distinguish between hepatitis-like (hepatocellular) and bile-blockage (cholestatic) patterns. It is calculated by dividing the ALT ratio by the ALP ratio. R > 5 is hepatocellular, R < 2 is cholestatic.
What to Do Next
If you are starting a long course of antibiotics and have a history of liver issues, ask your doctor for a baseline liver function test. If you notice a sudden change in the color of your skin or urine, contact your provider immediately. For those in a caregiving role for an ICU patient, keep a log of when new antibiotics are introduced, as this helps clinicians pinpoint the cause if liver enzymes start to climb.





Del Bourne
April 6, 2026 AT 19:08 PMIt is so important to keep an eye on those LFTs when starting a long course. I've seen many cases where patients felt completely fine while their ALT was skyrocketing, which is why that baseline test is a lifesaver for early detection.
Benjamin cusden
April 8, 2026 AT 16:47 PMThe mention of the R-ratio is basic clinical knowledge, yet it's fascinating how many people genuinely don't grasp the distinction between hepatocellular and cholestatic patterns. Most laypeople just see 'liver damage' as a monolithic entity, ignoring the nuanced biochemical differences that dictate the entire treatment protocol.
jack hunter
April 9, 2026 AT 23:51 PMprobly just the body rejecting the poison we call medicine... its funny how we trust these pills blindly until our liver starts melting. the whole system is just a loop of fixin one thing and breakin another lol
Vivek Hattangadi
April 10, 2026 AT 09:28 AMThis is such a helpful breakdown! I really think the part about probiotics and Faecalibacterium prausnitzii is the most exciting bit here. If we can actually protect the gut barrier, we can potentially avoid these liver spikes altogether. Great way to look at preventative care!
Windy Phillips
April 10, 2026 AT 17:08 PMSome people actually think they can just 'notice' jaundice before a doctor tells them... how quaint... I suppose we're all just waiting for our livers to fail in a perfectly timed fashion!!!
Srikanth Makineni
April 12, 2026 AT 04:14 AMjust check the labs
Daniel Trezub
April 12, 2026 AT 12:19 PMActually, the 7-day risk increase is a bit overblown if you consider the baseline severity of the infections being treated. I mean, sure, the risk goes up, but you're not exactly choosing between a 3-day and 7-day course for a mild cold when you're in the ICU.
Kathleen Painter
April 13, 2026 AT 23:35 PMI really appreciate how this post brings up the gut-liver axis because it encourages us to think about our bodies as interconnected systems rather than just isolated organs. It's so easy to forget that what happens in our intestines directly impacts our hepatic health, and while the science of mitochondrial dysfunction sounds scary, it actually gives us a roadmap for how to better support our bodies through nutrition and mindful supplementation during these tough medication cycles. I've always believed that a holistic approach, combining the necessary pharmaceutical interventions with a focus on microbiome diversity, is the only way we will truly move past the 'trial and error' phase of antibiotic prescribing, especially when you consider how genetic predispositions like HLA markers play such a massive role in individual reactions. It's just a beautiful reminder that everyone's biology is unique and deserves a tailored approach to medicine.
Christopher Cooper
April 15, 2026 AT 02:16 AMThe possibility of genetic testing for antibiotic sensitivity is a total game-changer! Imagine a world where you don't have to gamble with your liver health just to clear an infection. This kind of personalized medicine is exactly where we need to be heading.
Darius Prorok
April 16, 2026 AT 08:06 AMI knew about the R-ratio. It's just math. You divide one number by another and it tells you what's wrong. Not that hard.
Timothy Burroughs
April 17, 2026 AT 14:50 PMTypical government medical nonsense telling you to get tests first everything is just a money grab and they dont even care that real men can handle a bit of liver stress if it means killing the bugs
Alexander Idle
April 17, 2026 AT 18:20 PMThe audacity of these pharmaceutical companies to sell us drugs that effectively sandpaper our internal organs is simply theatrical. It is a tragedy of the highest order that we must rely on such crude instruments for healing!
Ruth Swansburg
April 19, 2026 AT 00:30 AMStay strong everyone! Monitoring is key.
Dhriti Chhabra
April 20, 2026 AT 06:17 AMI believe a collaborative approach between patients and physicians regarding baseline testing would greatly reduce the incidence of severe hepatic complications.
Rupert McKelvie
April 21, 2026 AT 00:44 AMIt's great that we're seeing more research into the gut microbiome. There's a lot of hope for the future of medicine here!