TNF Inhibitor Safety & Screening Guide
Select the specific TNF inhibitor medication you have been prescribed.
The critical window for preventing TB reactivation.
Screening Phase
Before starting therapy. IGRA or TST testing is mandatory. If positive, do not start drug yet.
Latent Treatment (If Positive)
Treat LTBI for at least 1 month before starting the biologic. Standard course is 4-9 months.
High Risk Window
Months 1–6 of therapy. Most reactivations occur here. Vigilance is critical.
Always consult your physician for medical advice.
Required Screening Steps
Symptoms to Watch For
Report these immediately to your doctor, especially in the first 6 months.
Imagine you have just been prescribed a powerful new medication to stop the pain of rheumatoid arthritis or psoriasis. It’s a biologic drug called a TNF inhibitor, which is a class of biologic medications that suppress inflammation by blocking tumor necrosis factor-alpha (TNF-α). You are excited because this medicine can change your life. But there is a hidden danger lurking in the shadows of this therapy. By calming down your immune system, these drugs also lower its guard against an old enemy: tuberculosis (TB), which is a bacterial infection caused by Mycobacterium tuberculosis that primarily affects the lungs but can spread to other organs. Specifically, TNF inhibitors can wake up latent tuberculosis infections that have been sleeping in your body for years.
This isn’t just theoretical fear. The risk is real, measurable, and varies significantly depending on which specific drug you take. Understanding how to screen for this risk and monitor your health while on therapy is not optional-it is essential for staying safe. Let’s look at why this happens, which drugs carry the highest risk, and exactly what steps you need to take before and during treatment.
Why TNF Inhibitors Wake Up Sleeping TB
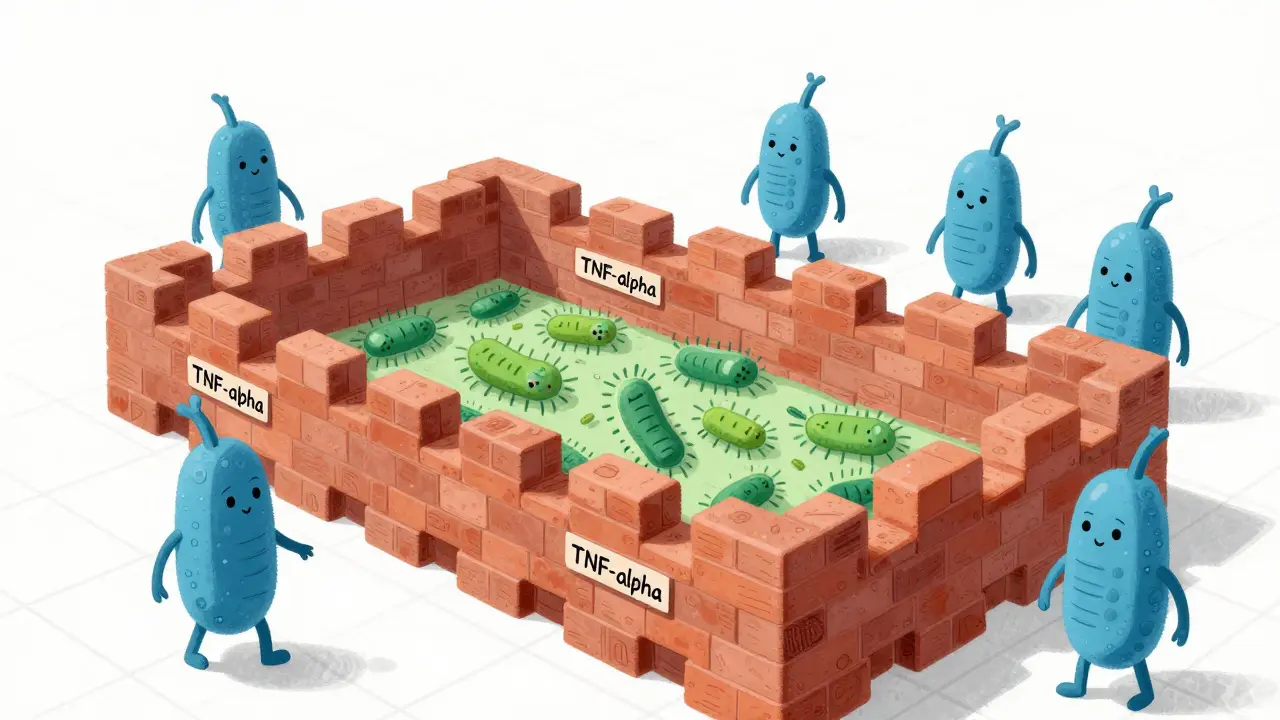
To understand the risk, we first need to look at how your body fights tuberculosis naturally. When you breathe in TB bacteria, your immune system tries to contain them. It builds tiny walls around the bacteria using immune cells. These structures are called granulomas. Think of them as prison cells built by your white blood cells to keep the TB bacteria locked away. As long as the wall holds, you have latent tuberculosis infection (LTBI), meaning you carry the bacteria but do not get sick.
The problem arises because tumor necrosis factor-alpha (TNF-α) is the cement that holds those granuloma walls together. TNF inhibitors work by blocking this protein to reduce inflammation in conditions like rheumatoid arthritis, ankylosing spondylitis, and inflammatory bowel disease. However, when you block TNF-α, you weaken the granulomas. The "prison walls" crumble, allowing the dormant TB bacteria to escape, multiply, and cause active disease. This process is known as TB reactivation.
Not all TNF inhibitors break down these walls equally. Research shows a clear difference in risk based on how the drug binds to the TNF protein. Drugs that bind only to soluble TNF leave membrane-bound TNF alone, preserving some granuloma integrity. Drugs that bind to both forms strip away more protection, leading to higher risks.
Different Drugs, Different Risks
If you are starting therapy, knowing which specific medication you are taking matters immensely for your TB risk profile. The British Society for Rheumatology Biologics Register (BSRBR) study provided crucial data here, showing that not all biologics are created equal regarding tuberculosis safety.
| Drug Name | Type | Relative TB Risk | Mechanism Detail |
|---|---|---|---|
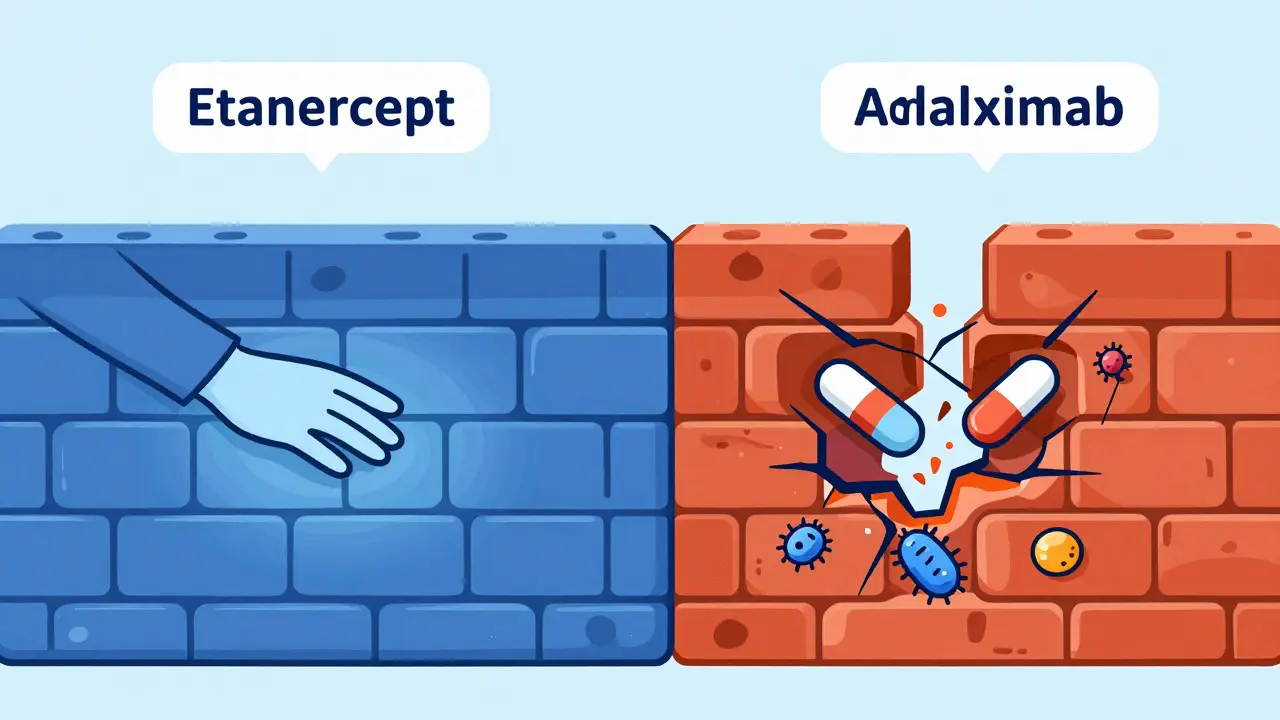
| Etanercept (Enbrel) | Soluble Receptor (Class 1) | Lowest | Binds only soluble TNF; preserves membrane-bound TNF function. |
| Adalimumab (Humira) | Monoclonal Antibody (Class 2) | High | Binds both soluble and membrane-bound TNF; disrupts granuloma integrity. |
| Infliximab (Remicade) | Chimeric Monoclonal Antibody (Class 3) | High | Binds both soluble and membrane-bound TNF; similar high risk to adalimumab. |
Studies consistently show that patients taking infliximab or adalimumab face a more than three-fold higher incidence of incident tuberculosis compared to those taking etanercept. In one recent retrospective study of over 500 patients, adalimumab showed a particularly elevated risk despite most patients receiving preventive treatment. This means if you are prescribed Humira or Remicade, your vigilance regarding TB must be stricter than if you were on Enbrel.
Screening Protocols: What Happens Before You Start?
Because the stakes are so high, expert consensus from organizations like the American Thoracic Society and the Centers for Disease Control and Prevention mandates universal screening for latent tuberculosis infection before you ever receive your first dose of a TNF inhibitor. You cannot skip this step.
There are two main tests used for this screening:
- Tuberculin Skin Test (TST): Also known as the PPD test, this involves injecting a small amount of fluid under your skin and checking for a reaction after 48-72 hours. It is widely available but can sometimes yield false positives if you have received the BCG vaccine (common in many countries outside the US).
- Interferon-Gamma Release Assay (IGRA): This is a blood test (such as QuantiFERON-TB Gold). It is often preferred because it is more specific and not affected by prior BCG vaccination. Recent guidelines suggest IGRA as the primary tool, especially for patients from high-TB-burden regions.
If your test comes back positive, indicating latent TB, you generally should not start the TNF inhibitor immediately. Instead, you begin treatment for the latent infection. The standard regimen has historically been isoniazid taken daily for nine months. However, adherence to this long course is difficult, with nearly a third of patients stopping due to side effects like liver toxicity concerns. Fortunately, newer regimens are changing this landscape. In 2024, the FDA approved a shorter four-month combination of rifampin and isoniazid, which has improved completion rates significantly.
Guidelines typically recommend completing at least one month of LTBI treatment before starting the biologic. For patients from high-TB-burden countries (defined as having more than 40 cases per 100,000 people annually), some European guidelines even recommend treating for latent TB regardless of the initial screening result, due to the higher likelihood of exposure.
Monitoring During Therapy: Staying Vigilant
Getting a negative screening result does not give you a lifetime pass. False negatives happen, and you can acquire a new TB infection while on therapy. Therefore, monitoring continues throughout your treatment.
Your healthcare provider will likely ask you to report any symptoms immediately. Be hyper-aware of the classic signs of TB, which include:
- Persistent cough lasting more than three weeks
- Fever, chills, or night sweats
- Unexplained weight loss
- Fatigue or general weakness
A critical detail to remember is that TB associated with TNF inhibitors often presents differently than typical community-acquired TB. While lung involvement is common, studies show that nearly 80% of these cases involve extrapulmonary sites-meaning the infection spreads to lymph nodes, bones, kidneys, or the central nervous system. This makes diagnosis harder because you might not have a cough. If you develop swollen lymph nodes or bone pain, tell your doctor right away.
The majority of reactivation cases occur within the first three to six months of starting therapy. This is your highest-risk window. After the first year, the risk decreases but never disappears completely. Annual symptom checks are recommended for as long as you remain on the biologic.

What If TB Develops? Handling Complications
If active TB is diagnosed while you are on a TNF inhibitor, the management becomes complex. First, the biologic drug is usually stopped immediately. Second, you begin a multi-drug antibiotic regimen for active TB, which lasts much longer than the latent treatment-typically six to nine months.
A unique complication in this scenario is TB-IRIS, or Tuberculosis Immune Reconstitution Inflammatory Syndrome. This occurs when your immune system starts recovering (either from stopping the biologic or starting TB meds) and reacts violently to the dead or dying bacteria. It causes severe inflammation that can mimic worsening TB. Paradoxically, doctors may need to use steroids to calm this immune storm while continuing antibiotics. This requires careful coordination between your rheumatologist, pulmonologist, and infectious disease specialist.
It is also worth noting that mortality rates for anti-TNF-associated TB are about 23% higher than for regular community TB. This underscores why early detection through rigorous screening and prompt reporting of symptoms is so vital.
Future Directions and Safer Options
Science is moving forward to address this inherent flaw in current biologics. Researchers are working on next-generation TNF inhibitors that selectively target soluble TNF without affecting membrane-bound TNF. Early Phase II trials of these selective agents, such as CD271-targeted therapies, have shown an 80% reduction in TB reactivation risk in animal models compared to conventional drugs like adalimumab. While these are not yet widely available, they represent a promising future where you can treat autoimmune diseases without sacrificing your defense against tuberculosis.
In the meantime, biosimilar versions of existing drugs like adalimumab have become more affordable, reducing the financial barrier to care. However, the biological mechanism remains the same, so the TB risk profile does not change with biosimilars. You still need the same level of screening and caution.
Can I take TNF inhibitors if I had TB in the past?
Yes, but with strict precautions. If you have completed full treatment for active TB in the past, you can often safely take TNF inhibitors. Your doctor will likely require chest X-rays and clinical evaluation to ensure the previous infection is fully cured and inactive before starting therapy. You will also need closer monitoring for any signs of recurrence.
Is the TB skin test enough, or do I need a blood test?
While the Tuberculin Skin Test (TST) is acceptable, the Interferon-Gamma Release Assay (IGRA) blood test is often preferred, especially if you have had the BCG vaccine. IGRA is more specific and reduces false-positive results. Many experts now recommend IGRA as the primary screening tool for patients starting biologic therapy.
How long do I need to wait after LTBI treatment before starting my biologic?
Current guidelines generally recommend waiting until you have completed at least one month of latent TB treatment before initiating TNF inhibitor therapy. Some specialists prefer to wait until the full course is finished, but starting the biologic after one month is considered safe in many protocols to avoid delaying autoimmune treatment unnecessarily.
Does Etanercept have the same TB risk as Humira?
No, Etanercept carries a significantly lower risk of TB reactivation compared to Humira (adalimumab) or Remicade (infliximab). This is because Etanercept acts as a soluble receptor that binds only soluble TNF, leaving membrane-bound TNF intact, which helps maintain the granuloma structures that contain TB bacteria.
What should I do if I develop a cough while on Adalimumab?
If you develop a persistent cough, fever, night sweats, or unexplained weight loss while taking Adalimumab, contact your healthcare provider immediately. Do not wait for your next scheduled appointment. These could be signs of TB reactivation or another serious infection. Your doctor may pause your biologic therapy and order chest imaging and sputum tests to rule out tuberculosis.

Diana Wiechecka
May 19, 2026 AT 17:10 PMWow, this explains so much! 😲 I was always confused why my doctor made me do the blood test instead of the skin prick. Thanks for clarifying the BCG issue! 🩸✨
Kathryn Byrd
May 19, 2026 AT 23:27 PMIn many countries where TB is endemic, the distinction between latent and active infection can be quite blurred due to high exposure rates. The guidelines mentioned here align with what we see in clinical practice regarding IGRA preference over TST to avoid false positives from childhood vaccination.
Tanya KLIMCHUK Klimchuk
May 20, 2026 AT 12:21 PMListen up, folks! If you are taking Humira or Remicade, you need to be vigilant! Do not ignore symptoms! It is not worth risking your life for convenience! Get screened properly! Stop being lazy about your health! This information could save your life, so pay attention!
Anthony Red
May 20, 2026 AT 13:20 PMHey everyone, good info here. Just wanted to add that if you have family history of TB, you should definitely mention that to your rheumatologist before starting anything. Better safe than sorry, right? 👍
Javier Arauz
May 20, 2026 AT 22:37 PMWhy are we even using these drugs? They are dangerous garbage. We should stick to traditional treatments that don't cripple your immune system. This is another example of big pharma pushing risky meds without caring about long-term consequences like TB outbreaks. Unacceptable.
Kris Wong
May 22, 2026 AT 11:04 AMThe government knows exactly what they are doing with these screenings. It is all about data collection and control. They want to track who has latent TB to monitor population movements. Don't trust the FDA approvals blindly! 🚫👁️
Danny S
May 22, 2026 AT 23:24 PMIt is obvious that the pharmaceutical industry benefits from keeping patients on lifelong biologic therapy rather than curing them. The TB risk is a convenient way to keep doctors involved and monitoring compliance. Wake up sheeple! 😡
Jeremiah Cassandra
May 24, 2026 AT 14:20 PMAh yes, nothing says 'safe medical treatment' like potentially waking up a sleeping bacterial monster in your lungs. Thanks for the tip on Etanercept though, at least there is one option that doesn't sound like a horror movie plot. 🙄💉
charles robert
May 26, 2026 AT 07:05 AMThe human body is a complex prison, and we are merely the wardens failing to maintain the walls. When we block TNF, we are essentially breaking down the bars of our own cellular jails. It is a profound metaphor for the fragility of existence. Why do we seek to suppress inflammation when it is the very fire that keeps the darkness at bay? 🌑🔥
Warren Brewer
May 26, 2026 AT 13:03 PMGood post. Simple terms help. I tell my patients to watch for coughs. If you get sick, call your doctor. Do not wait. It is important to know your drug type too. Some are riskier than others.