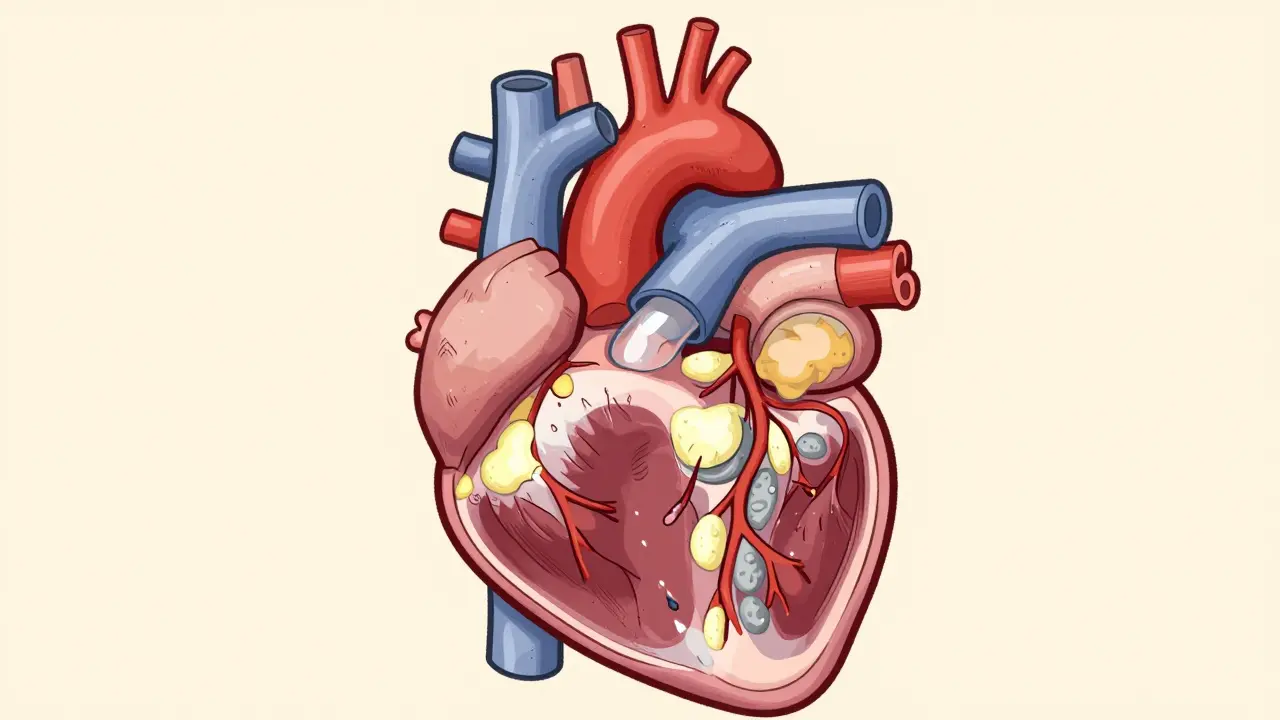
Imagine your heart’s blood supply lines slowly clogging up, like pipes in an old house gathering sediment over decades. That is exactly what happens with Coronary Artery Disease, commonly known as CAD or ischemic heart disease. It is the leading cause of death globally, accounting for roughly 13% of all fatalities worldwide between 2000 and 2021 according to World Health Organization data. The condition isn’t just about chest pain; it is a systemic issue where the arteries that feed your heart muscle narrow and harden, restricting oxygen-rich blood flow.
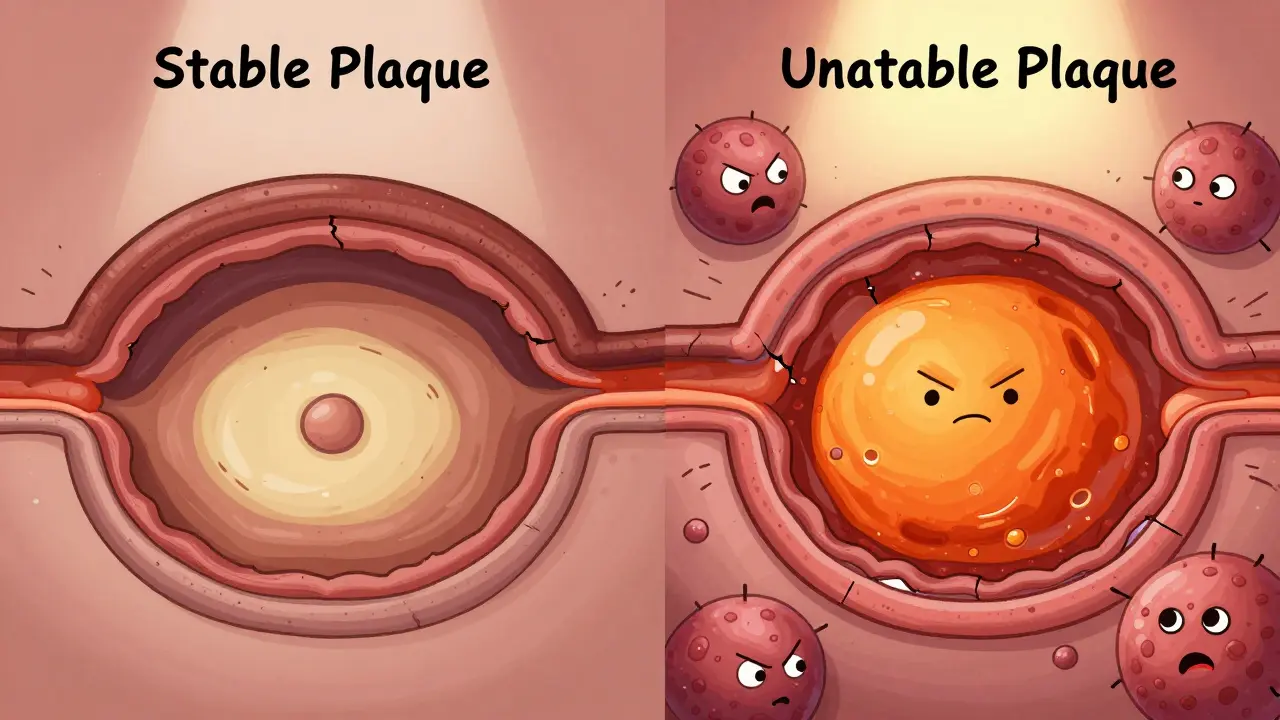
The root cause of this narrowing is atherosclerosis. This process involves the buildup of fatty deposits, cholesterol, and other substances-collectively called plaque-inside your arterial walls. Over time, these plaques can calcify and become fibrous, turning flexible arteries into rigid tubes. While stable plaques might gradually narrow the vessel lumen by more than 50%, causing predictable symptoms during exercise, unstable plaques are far more dangerous. These unstable formations often have thin fibrous caps and large lipid cores. Paradoxically, they may narrow the artery by less than 50% but can rupture suddenly, triggering a blood clot that causes a heart attack.
How Atherosclerosis Develops in Your Heart
Atherosclerosis does not happen overnight. It is a slow-moving process driven by inflammation and endothelial dysfunction-the lining of your blood vessels gets damaged, often due to high blood pressure or smoking. Once the inner layer is injured, low-density lipoprotein (LDL) particles, often referred to as "bad" cholesterol, seep into the arterial wall. Inflammatory cells, specifically macrophages, rush to the site to clean up the LDL, but they end up becoming part of the problem. They ingest the cholesterol and turn into foam cells, which accumulate to form the core of the plaque.
As this process continues, smooth muscle cells proliferate and create a fibrous cap over the lipid core. If this cap remains thick and strong, the plaque is considered stable. However, if the cap is thin and the lipid core is large, the plaque becomes vulnerable. When such a plaque ruptures, the body treats it like an injury, sending platelets to seal the breach. This rapid clotting can completely block the coronary artery, cutting off blood supply to the heart muscle and resulting in myocardial infarction.
Identifying Your Risk Profile
Not everyone faces the same level of danger from CAD. Doctors now use sophisticated risk stratification models to categorize patients into Low Risk (<1% yearly risk), Intermediate Risk (1% to 3%), and High Risk (>3%) for cardiovascular death or nonfatal heart attack. This shift toward personalized assessment was highlighted in the 2023 ACC/AHA Chronic Coronary Disease Guidelines. Understanding where you fall on this spectrum helps determine how aggressive your treatment needs to be.
Several key factors push you into higher risk categories:
- Diabetes: High blood sugar damages blood vessels and nerves that control them, significantly accelerating atherosclerosis.
- Dyslipidemia: Elevated levels of LDL cholesterol and triglycerides provide the raw material for plaque formation.
- Hypertension: High blood pressure strains the arterial walls, creating entry points for cholesterol.
- Smoking: Tobacco use causes immediate damage to the endothelium and increases clotting tendency.
- Chronic Kidney Disease: An estimated glomerular filtration rate (eGFR) below 60 ml/min is a major red flag, as kidney function closely mirrors vascular health.
- Prior Events: A history of myocardial infarction, percutaneous coronary intervention (PCI), or coronary artery bypass grafting (CABG) places you in a higher bracket automatically.
Interestingly, research indicates that while only a portion of the population exhibits high-risk features, approximately 75% of primary cardiovascular events occur within this high-risk group. This underscores why identifying these markers early is crucial for prevention.
| Feature | Stable Plaque | Unstable Plaque |
|---|---|---|
| Fibrous Cap Thickness | Thick | Thin |
| Lipid Core Size | Small | Large |
| Inflammatory Cells | Few | High Macrophage Content |
| Vessel Narrowing | Often >50% | Often <50% |
| Symptoms | Predictable angina on exertion | Unpredictable, can cause sudden heart attack |
Diagnosing Coronary Artery Disease
You cannot always feel atherosclerosis progressing. Many people live with significant narrowing without any symptoms until a critical event occurs. Diagnosis typically begins with non-invasive tests. An electrocardiogram (ECG) records the electrical activity of your heart and can reveal signs of past damage or current strain. Stress tests evaluate how your heart performs under physical activity, looking for changes in rhythm or blood flow that indicate ischemia.
If initial tests suggest issues, doctors may order a coronary angiography. This invasive procedure involves threading a catheter through an artery in your wrist or groin up to your heart. Contrast dye is injected, allowing X-ray visualization of the coronary arteries. This gold-standard test precisely maps out blockages and their severity. Additionally, because peripheral artery disease (PAD) often coexists with CAD, an Ankle-Brachial Index (ABI) test is frequently recommended to check for circulation problems in the legs, providing a broader picture of your vascular health.

Treatment Strategies: From Lifestyle to Surgery
Managing CAD requires a multifaceted approach tailored to your specific risk profile. The goal is twofold: relieve symptoms and prevent future heart attacks. Treatment generally falls into three buckets: lifestyle changes, medication, and procedural interventions.
Lifestyle Modifications form the foundation of care. This means adopting a heart-healthy diet rich in fruits, vegetables, whole grains, and lean proteins while reducing saturated fats and sodium. Regular aerobic exercise improves circulation and helps manage weight and blood pressure. Quitting smoking is arguably the single most impactful change you can make, as it immediately reduces inflammation and clotting risk.
Medications are essential for most patients, especially those with established disease. Statins lower LDL cholesterol and stabilize existing plaques, preventing rupture. Antiplatelet agents like aspirin or clopidogrel keep blood cells from sticking together and forming clots. Beta-blockers and ACE inhibitors reduce the workload on the heart and lower blood pressure. For patients with atrial fibrillation, anticoagulants may also be necessary to prevent stroke, requiring careful balancing with antiplatelet therapy as outlined in recent guidelines.
When lifestyle and drugs aren't enough, or when blockages are severe, Procedural Interventions come into play. Percutaneous Coronary Intervention (PCI), commonly known as angioplasty and stenting, opens narrowed arteries using a balloon and a mesh tube called a stent. This minimally invasive procedure restores blood flow quickly. For complex cases involving multiple blocked vessels or left main coronary artery disease, Coronary Artery Bypass Grafting (CABG) surgery may be required. Surgeons take a healthy blood vessel from another part of your body and attach it to the coronary artery, creating a detour around the blockage.
Emerging Trends and Future Directions
The landscape of cardiac care is evolving rapidly. One significant development is the rise of cardio-oncology. As cancer survival rates improve and populations age, more patients are living with both chronic coronary disease and cancer. Treating one condition can sometimes exacerbate the other, necessitating specialized management strategies that balance chemotherapy risks with heart health.
Furthermore, the focus is shifting toward precision medicine. Instead of a one-size-fits-all approach, doctors are using genetic markers and detailed risk scores to tailor therapies. The 2023 guidelines emphasize thorough risk assessment to optimize outcomes, moving away from reactive treatment to proactive prevention. Research into plaque stabilization techniques continues, aiming to identify and treat vulnerable plaques before they rupture, potentially changing how we intervene in the future.
What is the difference between coronary artery disease and atherosclerosis?
Atherosclerosis is the underlying process where plaque builds up inside arteries, causing them to harden and narrow. Coronary artery disease is the specific result of atherosclerosis occurring in the coronary arteries that supply blood to the heart. You can think of atherosclerosis as the mechanism and CAD as the condition affecting the heart.
Can coronary artery disease be reversed?
While advanced calcified plaque cannot be fully removed without surgery, the progression of CAD can be halted and even partially reversed through aggressive lifestyle changes and medication. Lowering LDL cholesterol significantly can help shrink soft plaque components and stabilize existing deposits, reducing the risk of heart attack.
Why are unstable plaques more dangerous than stable ones?
Unstable plaques have thin fibrous caps and large lipid cores. They are prone to rupturing suddenly, which triggers immediate blood clot formation that can completely block the artery. Stable plaques, although they may narrow the artery more, usually do so gradually, giving the body time to adapt and causing predictable symptoms rather than sudden catastrophic events.
What does a high-risk score mean for my treatment?
A high-risk score (greater than 3% yearly risk of cardiovascular death or nonfatal MI) indicates that you need more intensive therapy. This might include stronger statins, dual antiplatelet therapy, stricter blood pressure targets, and possibly earlier consideration for surgical interventions like CABG or PCI to prevent a major cardiac event.
How does diabetes increase the risk of heart disease?
High blood sugar levels damage the inner lining of blood vessels (endothelium) and promote inflammation. This makes it easier for cholesterol to build up and form plaque. Diabetes also affects nerve signals that control heart rate and blood vessel dilation, making the heart work harder and increasing the likelihood of complications.



Sean Luke
I specialize in pharmaceuticals and have a passion for writing about medications and supplements. My work involves staying updated on the latest in drug developments and therapeutic approaches. I enjoy educating others through engaging content, sharing insights into the complex world of pharmaceuticals. Writing allows me to explore and communicate intricate topics in an understandable manner.
view all posts