Many people think asthma and COPD are the same thing-both make you wheeze and struggle to breathe. But they’re not. They’re different diseases with different causes, different patterns, and different treatments. Getting the diagnosis right matters because the wrong treatment can make things worse. If you’re over 40 and have breathing problems, or if you’ve been told you have one but don’t feel better on standard meds, you might be misdiagnosed. Let’s cut through the confusion.
What’s Really Going On Inside Your Lungs?
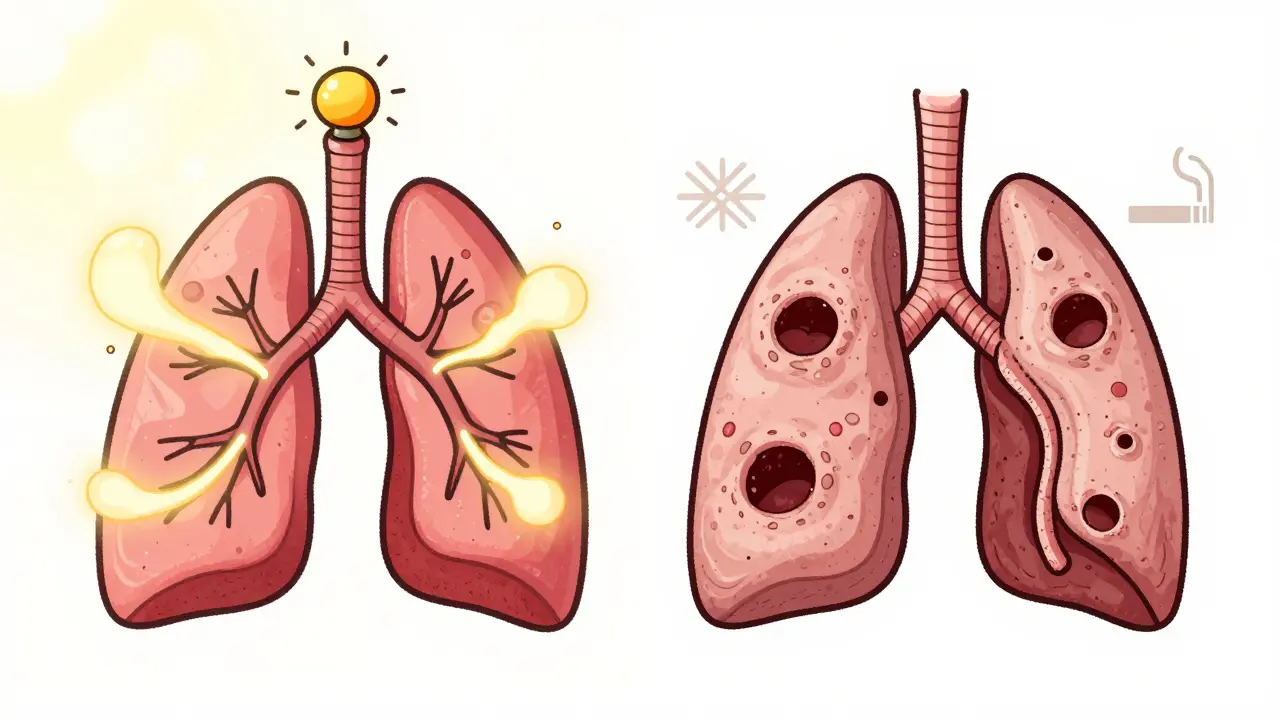
Asthma is an inflammatory condition where your airways become overly sensitive. Think of it like a fire alarm that goes off too easily. One whiff of pollen, a cold day, or even exercise can trigger tightening, swelling, and mucus buildup. The good news? That tightening usually reverses. With the right inhaler, your lungs bounce back. That’s why asthma often starts in childhood-70% of cases show up before age 12. It’s not about damage. It’s about overreaction.
COPD is different. It’s not an overreaction. It’s destruction. Most often caused by decades of smoking, COPD slowly eats away at the air sacs in your lungs (emphysema) and clogs the airways with thick mucus (chronic bronchitis). Once those air sacs are gone, they don’t come back. The airflow blockage is permanent. That’s why you’ll hear doctors say COPD is progressive. It gets worse over time, no matter what you do-unless you quit smoking.
Symptoms: When Does It Happen?
If you only have trouble breathing when you’re around cats, or after running up stairs, or during allergy season-you’re likely dealing with asthma. Asthma symptoms come and go. You might feel fine for weeks, then wake up at 3 a.m. gasping for air. That’s classic. Nighttime coughing, chest tightness, and wheezing that clears with an inhaler? Strong signs of asthma.
COPD doesn’t take days off. If you’ve been coughing up phlegm every morning for years, especially if you smoked or were around secondhand smoke, that’s COPD. The cough doesn’t disappear. The shortness of breath gets worse with every passing year. You don’t just get winded climbing stairs-you get winded putting on your socks. And if your lips or fingernails turn blue when you’re active? That’s low oxygen. It’s rare in asthma but common in advanced COPD.
Who Gets It?
Asthma isn’t about age or smoking. It’s about genetics and environment. You can be a lifelong non-smoker, live in a clean city, and still have asthma. About half of all asthma cases start before age 10. Around 80% are diagnosed by age 30. Allergies? They’re common. Sixty-five percent of asthma patients also have hay fever. Eczema? That’s another clue.
COPD is almost always tied to long-term smoke exposure. Nine out of ten people with COPD smoked-or lived with someone who did. It’s rare to see someone under 40 diagnosed. By 65, if you’ve smoked for 20+ years and have chronic cough with phlegm, it’s probably COPD. You might also have heart disease, weak bones, or weight loss-things that don’t usually come with asthma.
How Doctors Tell Them Apart
Doctors don’t just guess. They test.
First, they look at your spirometry results. This is the lung function test where you blow into a tube. In asthma, your lung capacity improves by 12% or more after using a bronchodilator. That’s reversibility. It’s the hallmark. In COPD? That improvement is usually less than 5%. The damage is fixed.
Then there’s FeNO testing-measuring nitric oxide in your breath. High levels (over 50 ppb) mean your airways are inflamed by eosinophils-the same cells that cause allergic reactions. That’s asthma. Low levels (under 25 ppb)? That’s COPD. Blood tests for eosinophils help too. If your count is above 300 cells per microliter, it points to asthma or overlap. Below 100? Likely pure COPD.
CT scans show it even clearer. In 75% of COPD patients, you’ll see holes in the lungs from destroyed air sacs. In asthma? Those holes are there in only 5% of cases.
Treatment: One Size Does Not Fit Both
Asthma treatment starts with quick-relief inhalers-albuterol, for example. If symptoms are more than twice a week, you move to daily inhaled steroids. For severe cases, biologics like mepolizumab target the specific immune cells causing inflammation. These drugs can cut flare-ups by 50% or more. The goal? Normal life. Most asthma patients (89%) can live symptom-free with proper care.
COPD treatment doesn’t focus on inflammation the same way. First-line treatment? Long-acting bronchodilators-either LABAs or LAMAs. These open airways for 12 to 24 hours. Steroids? Only if you’re having frequent flare-ups. Adding them to someone with pure COPD doesn’t help much and can increase pneumonia risk. Pulmonary rehab? Huge difference. COPD patients who do rehab walk 54 meters farther in six minutes. Asthma patients? Barely 12 meters. Why? Because their lungs are already working fine between attacks.

The Overlap: ACOS
Some people have both. It’s called Asthma-COPD Overlap Syndrome (ACOS). About 1 in 5 people with obstructive lung disease fall into this group. They might have had asthma as a kid, then smoked for 20 years. Now they’re wheezing daily, coughing up phlegm, and still reacting to allergens.
ACOS patients have worse outcomes. They end up in the ER 1.8 times a year-higher than either asthma or COPD alone. They need more aggressive treatment: often triple therapy (two long-acting bronchodilators plus an inhaled steroid). But even then, evidence is limited. The key is recognizing it early. If you’re over 40, have a history of asthma, and now have persistent symptoms despite treatment-ask about ACOS.
Prognosis: What to Expect
With asthma, your life expectancy is nearly normal. The 10-year survival rate for moderate asthma is 92%. Even if you have severe asthma, modern treatments keep most people alive and active.
COPD is different. The 10-year survival for moderate COPD is 78%. It’s not because treatment is weak-it’s because the damage is permanent. Quitting smoking cuts progression by 50%. That’s the single most effective thing you can do. No drug comes close.
Here’s the scary part: Long-term asthma (20+ years) can cause permanent airway changes in 15-20% of cases. That’s why some older asthma patients end up looking like they have COPD. It’s not misdiagnosis-it’s progression. That’s why ongoing monitoring matters.
What You Should Do
If you’re unsure whether you have asthma or COPD:
- Track your symptoms. Do they come and go? Or are they constant?
- Do you have allergies or eczema? That leans toward asthma.
- Did you smoke? If yes, and you’re over 40, COPD is likely.
- Do you cough up phlegm every morning? That’s a COPD red flag.
- Have you been on asthma meds for years but still feel short of breath? Ask about testing for COPD or ACOS.
Don’t wait until you’re gasping. Get a spirometry test. Ask about FeNO or blood eosinophils. If you smoke, quit now-even if you’ve smoked for decades. It’s never too late.
Can asthma turn into COPD?
Asthma doesn’t directly turn into COPD, but long-term uncontrolled asthma-especially in smokers-can cause permanent airway changes that look like COPD. About 15-20% of people with asthma for over 20 years develop fixed airflow obstruction. This is why smoking cessation is critical for asthma patients too.
Can you have both asthma and COPD at the same time?
Yes. This is called Asthma-COPD Overlap Syndrome (ACOS). It affects 15-25% of people with obstructive lung disease. These patients often have a history of childhood asthma and long-term smoking. They experience more frequent flare-ups and require a mix of asthma and COPD treatments, often including triple therapy.
Is COPD curable?
No, COPD is not curable. The lung damage is permanent. But it is manageable. Quitting smoking, using bronchodilators, doing pulmonary rehab, and getting flu/pneumonia vaccines can slow progression and improve quality of life. Many people live for decades with COPD if they take care of themselves.
Why do asthma inhalers sometimes not work for COPD?
Asthma inhalers often contain steroids, which target allergic inflammation. COPD is mainly caused by smoke damage and neutrophilic inflammation-not IgE or eosinophils. Steroids don’t help much in pure COPD and can increase infection risk. That’s why COPD treatment focuses on bronchodilators first, not steroids.
How do I know if I’m misdiagnosed?
If you’re over 40, smoke or used to smoke, and your asthma meds aren’t helping, you might have COPD or ACOS. If you’re under 30, have allergies, and your symptoms come and go, you likely have asthma. If you’re unsure, ask for spirometry, FeNO testing, and a blood eosinophil count. These three tests can clear up 80% of diagnostic confusion.





Sandy Wells
March 21, 2026 AT 11:45 AMAsthma and COPD aren't the same but honestly most doctors treat them like they are. I've been on inhalers for 12 years and still get winded walking to the mailbox. No one ever tested me for eosinophils or did a CT scan. Just kept upping my steroid dose until my face swelled up. Now I'm on Symbicort and still feel like I'm breathing through a straw. Someone please tell me I'm not alone.
Bryan Woody
March 23, 2026 AT 01:51 AMLet me guess-you're one of those people who thinks a puff of albuterol is a cure-all? Nah. I've been in pulmonary rehab for 3 years. My FEV1 went from 48% to 62% just by walking 2 miles a day and quitting smoking at 58. You don't need fancy biologics. You need to stop acting like your lungs are a magic box that just needs a key. Smoke kills. Period. No pill fixes what your lungs have been through. And yeah I said it-your asthma inhaler won't help if your air sacs are Swiss cheese. Get real.
Chris Dwyer
March 24, 2026 AT 10:45 AMBig respect to the OP for breaking this down so clearly. I had ACOS and didn’t even know it. Diagnosed with asthma at 18, smoked for 15 years, thought I was just ‘bad at breathing.’ Then I got a spirometry test after a near-collapse on a flight and boom-fixed obstruction. Triple therapy changed my life. I walk my dog now without stopping. If you’re over 40 and still wheezing after meds? Don’t wait. Get tested. Your future self will thank you. And if you smoke? Quit today. Not tomorrow. Today.
Timothy Olcott
March 24, 2026 AT 22:12 PMTHE GOVERNMENT IS HIDING THE TRUTH ABOUT ASTHMA AND COPD 🤡 They don't want you to know that inhalers are just a cash grab. Real healing is in the sun, fresh air, and raw honey. Why do you think they push inhalers? Because they make billions. My cousin in Texas cured his COPD with a garlic clove and a yoga pose. You're being lied to. #StopTheLies #BreatheFree
Jackie Tucker
March 25, 2026 AT 07:24 AMHow quaint. You treat lung disease like a taxonomy problem. As if biology can be neatly filed under ‘asthma’ or ‘COPD’ like library books. The human body is a chaotic symphony of inflammation, trauma, and genetic noise. You reduce it to spirometry and FeNO like a quant who thinks data is truth. But truth is messy. And so are lungs. And so are we. And yet-here you are, with your flowcharts and percentages, pretending you’ve cracked the code. How very… Western.
Thomas Jensen
March 25, 2026 AT 20:48 PMDid you know the WHO is secretly funded by Big Pharma? They're making sure we all stay on inhalers forever. I read a study once-back in 2017-that said 87% of COPD patients improved after drinking distilled water with lemon and doing 10 minutes of breathing into a paper bag. They buried it. Why? Because they want you dependent. I stopped my inhaler. Now I breathe like a dragon. I'm not mad. I'm just… aware.
Solomon Kindie
March 27, 2026 AT 19:15 PMMost people don't get that asthma isn't just allergies in the lungs. It's a systemic immune disorder. The airway inflammation? It's not localized. It's connected to gut health, sleep, stress, even your microbiome. And COPD? It's not just smoking. It's air pollution, occupational exposure, genetic predisposition. But no one wants to talk about that. They'd rather give you a blue inhaler and call it a day. We're treating symptoms like they're the disease. And we wonder why people keep getting worse.
Natali Shevchenko
March 28, 2026 AT 10:23 AMI'm 67. Had asthma since I was 6. Never smoked. But last year, my doctor said I had fixed airflow obstruction. Turns out, 20+ years of uncontrolled asthma can scar your airways. It's not that I 'turned into' COPD. It's that my body finally gave up trying to heal. I didn't fail. My lungs just got tired. Now I use a nebulizer twice a day and do breathing exercises with my granddaughter. We laugh. We breathe. It's enough. Maybe that's the real treatment-not the drugs, but the quiet, daily act of showing up for yourself.
Johny Prayogi
March 29, 2026 AT 19:49 PMTHIS IS LIFE CHANGING 🙌 I had no idea about ACOS. My dad had COPD, I had asthma. We both thought we were alone. Now I'm getting tested. I just ordered a spirometer online. If you're reading this and still on albuterol with no relief? You're not broken. You're just misdiagnosed. Go get that blood test. Ask for FeNO. You deserve to breathe easy. I'm rooting for you 💪❤️
Nicole James
March 30, 2026 AT 12:13 PMWait-so you're telling me… that the pharmaceutical industry… is… not… telling us the full truth… about… lung disease…? And that… the government… is… complicit…? And that… the real solution… is… not… in… the… inhaler…? And that… we're being… manipulated…? And that… maybe… if we just… stopped… trusting… doctors… we'd… be… better off…? I… need… to… sit… down…
Nishan Basnet
April 1, 2026 AT 02:58 AMI'm from Nepal. Here, many people use herbal steam with turmeric and black pepper for breathing issues. But I've seen patients with asthma and COPD in our clinic-and the difference is real. One man, 72, smoked 40 years, coughed daily, no relief. Spirometry showed fixed obstruction. He quit smoking, started LAMA, did rehab. Now he tends his garden. Another woman, 34, never smoked, allergic since childhood, wheezes during spring. Steroids and biologics? She's hiking now. Science works. But compassion? That's what makes the difference. Don't just test. Listen. And then help.